The Business of Neurocritical Care: Understanding Risk Adjustment Factor (RAF) Scores and Their Impact on Reimbursement
Published on: March 22, 2024
In an earlier article in this series, I discussed the importance of provider documentation in the H&P, especially the documentation of Hierarchical Code Conditions (HCCs) tied to payments.
https://currents.neurocriticalcare.org/Leading-Insights/Article/the-business-of-neurocritical-care-how-your-docume
Recently, the Centers for Medicare and Medicaid Services (CMS) launched Version 28 of its HCCs when it published the “2024 Advance Notice with Proposed Payment Updates for the Medicare Advantage and Part D Prescription Drug Programs.” This version is based on claims data from 2016-2019 and is felt to be more accurate for current practice. It will have significant changes for the CMS-HCC Risk Adjustment Model for Contract Year 2024 which has already begun. Of note, the payment-related HCCs (those that are tied to reimbursement) increased from 86 to 115.
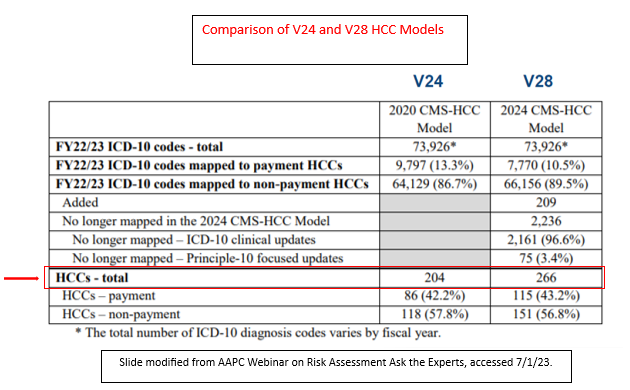
For 2023-2025, a blend of this new version (V28) and the prior version (V24) will be included in the models incorporating HCCs into the calculation of each patient’s RAF Score. However, before we jump into the important factors relevant to neurocritical care providers, let us define the elements of the RAF score.'
What is a RAF score?
RAF scores are used by CMS to estimate the cost of healthcare for a Medicare Advantage plan beneficiary for the upcoming year. It determines the monthly payment made by CMS to the health plan for a given beneficiary during the following year, also known as a contract year (CY). As such, the health plan will be paid at a higher rate for older patients with multiple medical conditions and with conditions of greater severity as the anticipated cost of care for the given patient will be higher (1). Risk adjustments were designed only for Medicare Advantage Plans, but their use is expanding as many healthcare systems are changing to value-based care (i.e., pay for performance).
How are RAF Scores Calculated?
RAF scores incorporate demographic data and disease risk scores. Demographic data includes age, sex, location of residence (home, skilled nursing facility, etc.) and disability status. Disease risk scores are determined from physical exam findings and diagnoses listed in provider documentation during face-to-face patient encounters (including synchronous telehealth encounters) and their associated HCCs. The lower the HCC number, the higher its contribution to the RAF score.
A RAF score of 1.00 means that the patient will have an average expected cost of care in the upcoming year. A score greater than 1.00 reflects a patient with a higher severity of illness while those below 1.00 are considered “healthier”. Given that the RAF score is greatly determined by provider documentation, it is imperative that the patient’s RAF score truly match the patient’s severity of illness as it will impact provider and organizational payments in the following year. In other words, the patient must look as sick on paper as they do in person in order for organizations and providers to be fairly reimbursed.
- Although the EHR has created efficiencies for providers such as auto-populated histories, problem lists, and diagnostic study results, it is important to note that none of these contribute to the RAF score as they do not count as being documented by the provider.
For example, if an auto-populated head CT report documents that the patient has a new large acute intraparenchymal hemorrhage, but the provider does not list it in their assessment and have a plan for it using at least one of the MEAT criteria (Monitor, Evaluate, Assess, Treat), it will not count as a diagnosis.
- It is best practice for providers to document each Diagnosis + Status + Treatment (plan) + Thought Process/Associated risk and conditions to enable coders to correctly capture the HCC and thus calculate a correct RAF score. (2)
The second key principle of coding, as discussed in the previous article, is that coders cannot infer anything that is not documented by a provider (especially from the history, medication list, problem list, diagnostic test results, or operative reports) unless discussed elsewhere in the physical exam or assessment/plan. For example, if the patient has a documented hemoglobin A1C of 12 in the lab section of the note and the medication list indicates that the patient is on an insulin infusion, coders cannot assume that this patient has uncontrolled Type II diabetes mellitus with hyperglycemia unless the provider uses those words as an assessment and documents a plan for it, such as “continue insulin infusion for now due to fluctuant glucose levels.”
Here I highlight certain changes that are germane to neurocritical providers. Of note, all sequelae codes were removed from the methodology, including spinal cord injuries. Therefore, one must document the functional state of the patient as a surrogate for the sequelae as shown below:
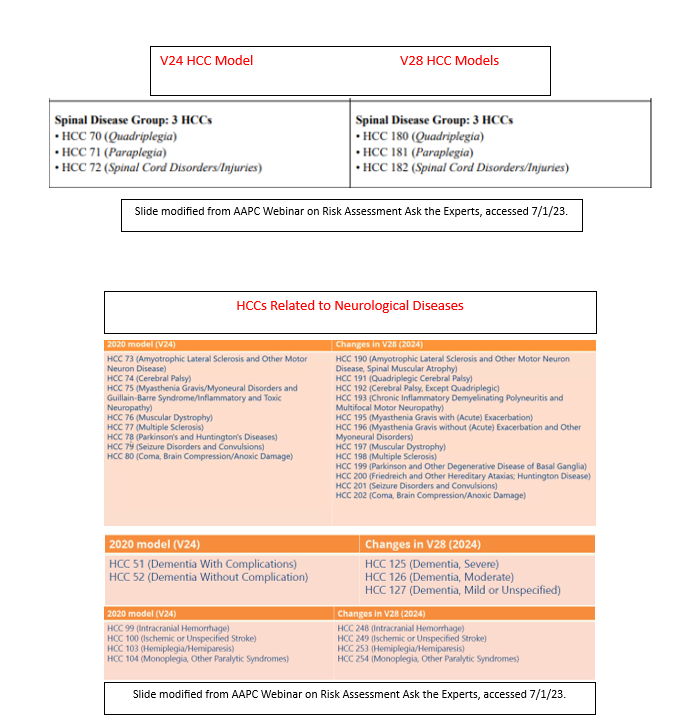
Documentation of dementia became much simpler, although the reimbursement decreased. Other common neurological conditions remained essentially unchanged with the exception of renumbering of the HCC (note that higher numbers mean lower reimbursement).
Certain conditions, although common to neurocritical care and clearly associated with high illness severity, were rarely documented overall and as such have been removed from the methodology. These include Guillain-Barre Syndrome, critical illness polyneuropathy, flexor posturing as best motor response in a comatose patient, and injury codes associated with sequelae of concussions. In addition, given the fact that the process is expected to reward high quality care, surgical complications such as intraoperative cerebrovascular infarction during surgery and post-procedural cerebrovascular infarction following cardiac surgery were removed from the HCC list.
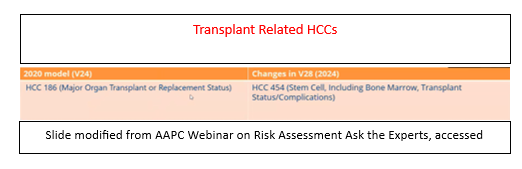
Three new additions relevant to NCC providers include diagnoses associated with liver disease (alcoholic hepatitis with or without ascites, toxic liver disease with chronic hepatitis, malignant ascites, etc.), any lower extremity amputation except toe amputations, and malignant pleural effusions. Also emphasized in V28 are the documentation of any type of transplant (including hematologic), as post-transplant states are clearly associated with greater cost.
The importance of correct documentation related to NCC is best illustrated in a recent Humana Insurance audit of a particular health system. In a review of 30 charts in which acute ischemic stroke was coded, there were zero that supported the diagnosis and thus the health system had to repay (with penalty) the money they had received as shown below:
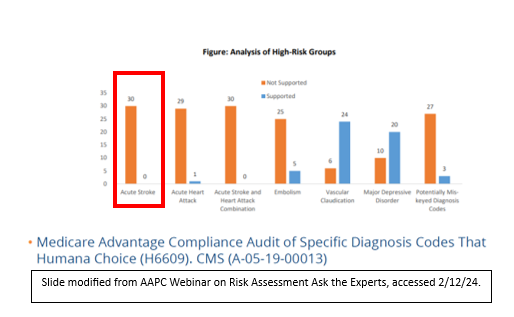
Although the details of this case are not known, it is possible that the patients identified in the audit may indeed have had acute ischemic strokes, but the provider may have used auto-populated radiology documentation (for example) to document the condition, which would not have been in compliance. Alternatively, perhaps they did not have an associated treatment plan documented.
Overall, as organizations shift towards value-based care and dig deeper into informatics to quantitate the cost of care provided, providers need to know that there is a possibility that their compensation may become individualized. For example, an NCC provider who documents well and captures the maximal amount of appropriate reimbursement for their health organizations may receive a higher salary than another NCC provider who takes care of a similar patient with the same length of stay and the same outcome, simply because of their documentation.