Point of Care Ultrasound-Guided Stellate Ganglion Block for Severe Vasospasm: An Option When Others are Limited
Published on: June 05, 2026
Clinical Case
A 23-year-old female with no known past medical history presented to the emergency department with subjective fevers, chills, generalized weakness, holocephalic headaches and photophobia. Her neurological exam was unremarkable. Her labs were notable for a white blood cell (WBC) count of 20K with neutrophilic predominance. Non contrast CT head was unremarkable. Given clinical concern for meningoencephalitis, she was empirically given vancomycin, ceftriaxone and acyclovir and underwent a lumbar puncture (LP). The LP had an opening pressure of 15cmH20, with polymorphonuclear pleocytosis, a normal glucose of 64 and an elevated protein of 70. The meningoencephalitis Biofire PCR, bacterial and fungal cultures were negative. On day one of hospitalization, her blood cultures grew Haemophilus Parainfluenza, and the antibiotic regimen was narrowed to ceftriaxone.
The transthoracic echo revealed severe mitral valve regurgitation (MR) with a mobile vegetation (Figure 1). She underwent CT angiogram of the head, neck, chest and abdomen that showed a left M4 segment mycotic aneurysm in the brain and multiple mycotic aneurysms in the liver. She then underwent a digital subtraction angiogram (DSA) that was complicated with the rupture of the L-M4 aneurysm while attempting to deploy glue, and an iatrogenic non-flow limiting dissection of the left petrous internal carotid artery, and severe catheter-induced vasospasm of the left middle cerebral artery (MCA), that was minimally responsive to intra-arterial vasodilators. Her post operative CTH showed a convexal subarachnoid hemorrhage (SAH) within the area of the ruptured mycotic aneurysm. CTA head re-demonstrated severe left MCA vasospasm. Nimodipine was initiated.
She became febrile with mixed septic and cardiogenic shock requiring vasopressors. She developed new aphasia with right hemiparesis. CTH and MRI were unchanged; no new ischemic strokes or hemorrhage. CTA demonstrated severe diffuse vasospasm of the distal left M1, and M2-M4 branches with hypoperfusion in the left MCA territory on CTP thought to be the cause of her neurologic decline. Treatment for her symptomatic vasospasm was limited as induced hypertension to augment cerebral perfusion pressure would compromise her tenuous hemodynamics in the setting of severe MR, and the severe catheter-induced vasospasm on prior DSA precluded further endovascular interventions. Cardiovascular surgery recommended urgent mitral valve repair; however, the risk of hypotension intra-op leading to elevated stroke risk was felt to outweigh the benefits.
A milrinone drip was started; however, almost immediately caused significant hypotension requiring maximum doses of norepinephrine to maintain MAP above 65mmHg. Therefore, milrinone was discontinued. A repeat CTA of the head showed persistent left MCA vasospasm. Her respiratory status deteriorated in the setting of flash pulmonary edema, and she was intubated for hypoxemic respiratory failure. With a limited neurologic exam and ongoing evidence of symptomatic vasospasm with limited options for treatment, she underwent a point of care ultrasound (POCUS) guided left stellate ganglion block (SGB).
Ten milliliters of 0.25% bupivacaine was injected into her left stellate ganglion. Within 24 hours her radiographic vasospasm on the CTA improved. The right sided weakness improved; however, she still had expressive aphasia.
Given the improvement of her radiographic vasospasm and strong indication for cardiac surgery, she successfully underwent a mitral valve repair, seven days after the diagnosis of clinically significant vasospasm. She was discharged from the hospital and was seen as an outpatient with near normal strength on the right side and improving aphasia.
Discussion
Evidence exists to support treating symptomatic vasospasm in aneurysmal SAH with blood pressure augmentation and endovascular balloon angioplasty or vasodilator therapy. [1,2,3]. In this case, augmenting blood pressure would make the pre-load dependent MR worse, and endovascular therapies were deferred given concern for iatrogenic injury.
The stellate ganglion carries sympathetic fibers to the head and neck region. It lies inferior to the common carotid artery, superior to the longus colli muscle at the level of C6-C7, and anterior to the transverse process and prevertebral fascia (Figure 2). With POCUS, using a linear probe, oriented in the transverse plane, perpendicular to the trachea, this anatomy can be visualized. To perform the block, a needle is inserted posterior to the carotid artery and superficial to the LG [4,5]. Local anesthetics -either lidocaine or bupivacaine- are injected slowly while observing the separation between the muscle and fascial layers as confirmation (Figure 3).
SGB has garnered attention in treating vasospasm over the past two decades. Although large, randomized control trials are lacking to confirm its efficacy, a systemic review looking into fifteen studies, involving 350 patients showed that the incidence of symptomatic vasospasm in patients treated with SGB decreased by 50% compared to controls [6]. We hereby demonstrate a case of an SBG block using POCUS to treat symptomatic vasospasm when conventional measures fail or are unsafe.
Figure 1: Apical 4-chamber view showing a mobile mass on the mitral valve.
Figure 2: Ultrasound of the stellate ganglion and surrounding structures.
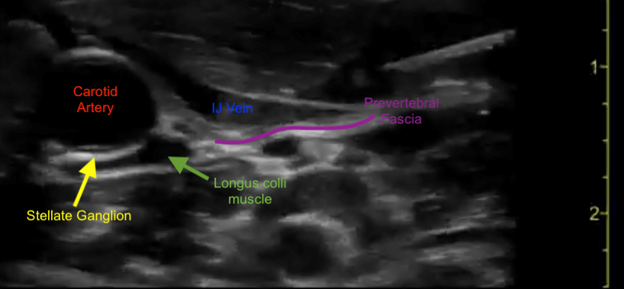
Figure 3: Injection of bupivacaine into the stellate ganglion.
References
1. Gathier, C. S., van den Bergh, W. M., van der Jagt, M., Verweij, B. H., Dankbaar, J. W., Muller, M. C., Oldenbeuving, A. W., Rinkel, G. J. E., Slooter, A. J. C., & HIMALAIA Study Group. (2018). Induced hypertension for delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage: A randomized clinical trial. Stroke, 49, 76–83. https://doi.org/10.1161/STROKEAHA.117.017956
2. Stuart, R. M., Helbok, R., Kurtz, P., Schmidt, M., Fernandez, L., Lee, K., Badjatia, N., Mayer, S. A., Lavine, S., Meyers, P., et al. (2011). High-dose intra-arterial verapamil for the treatment of cerebral vasospasm after subarachnoid hemorrhage: Prolonged effects on hemodynamic parameters and brain metabolism. Neurosurgery, 68, 337–345.
3. Biondi, A., Ricciardi, G. K., Puybasset, L., Abdennour, L., Longo, M., Chiras, J., & Van Effenterre, R. (2004). Intra-arterial nimodipine for the treatment of symptomatic cerebral vasospasm after aneurysmal subarachnoid hemorrhage: Preliminary results. American Journal of Neuroradiology, 25, 1067–1076.
4. Chang, K. V., Wu, W. T., & Özçakar, L. (2018). Ultrasound-guided interventions of the cervical spine and nerves. Physical Medicine and Rehabilitation Clinics of North America, 29(1), 93–103.
5. Narouze, S. (2014). Ultrasound-guided stellate ganglion block: Safety and efficacy. Current Pain and Headache Reports, 18(6), 424.
6. Ayaz, M., Sohail, H., Ibrahim, M., & Choufani, D. (2025). Evaluating the effectiveness of early stellate ganglion block in preventing vasospasm and delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage: A systematic review. Stroke: Vascular and Interventional Neurology, 5(Suppl. 1).