Point-of-Care Ultrasound Case Pearl in Neurocritical Care
Published on: April 06, 2018
Point-of-care ultrasound (POCUS) is ultrasonography performed by the provider in real time at the bedside to help clinical decision making. POCUS is increasingly being implemented as a powerful tool for screening, diagnosis, monitoring of critically ill patients as well as procedural guidance. POCUS complements the physical examination, improves immediate bedside therapeutic decision making, and optimizes the choice and the yield of further diagnostic testing.
Focused Assessment with Sonography for Trauma (FAST) examination is an ultrasound-driven evaluation of the torso indicated in patients after traumatic injury. The FAST exam maximizes the probability for early detection of pericardial, pleural and peritoneal free fluid (blood, urine or bile), which appears as a hypoechoic (i.e., black or dark gray) collection. The extended FAST exam (e-FAST) incorporates anterior-chest ultrasonography for the identification of pneumothorax. A recent study demonstrated that e-FAST, compared to computed tomography, demonstrated specificities of 100 percent for pneumothorax and 98.4 percent for peritoneal free fluid, but sensitivities of 100 percent, 75 percent and 42.9 percent for pleural effusion, pneumothorax and peritoneal free fluid, respectively.
Knowledge of practice guidelines for the performance of the FAST examination may be of great educational value to a neurointensivist even in non-traumatic cases. Using a low-frequency (2.5 to 5 MHz) curvilinear or phased-array transducer, the standard FAST exam consists of the following evaluations of the heart for pericardial fluid: right flank (hepato-renal view/Morison’s pouch), left flank (peri-splenic view) and pelvic (retro-vesical view) for peritoneal fluid and lateral and anterior thoracic views for hemothorax and pneumothorax, respectively. FAST may not be useful in patients with obesity, subcutaneous emphysema and lesions that produce smaller than 200 ml of free fluid (>200 ml) but in cases of acute traumatic shock can help identify free fluid and triage need for exploratory laparotomy.
We describe the use of FAST exam in a 68-year-old man with diagnosis of locked-in syndrome who underwent tracheostomy and percutaneous endoscopic gastrostomy. Upon return to the neurointensive care unit, the patient developed shock unresponsive to fluid resuscitation, consequently requiring vasopressor support. There was no drop in hemoglobin noted. With patients cardiac history presumed, cardiogenic shock was suspected. Increasing vasopressor requirements with worsening shock necessitated further assessment. The neurointensivist team performed POCUS of heart with parasternal long and short axis views showing normal gross biventricular function, mild pericardial effusion but no signs of tamponade physiology (Figure: 1 and 2) ruling out cardiogenic shock. An e-FAST exam revealed peritoneal free fluid in the hepato-renal and peri-splenic views (Figures 2 and 3), and absent hemothorax and pneumothorax. POCUS exam took approximately five minutes to complete. Emergency general surgery was contacted who took the patient for emergency laparotomy and found extensive mesenteric hematomas from a bleeding source related to peg tube placement. Successful control of source of bleeding was done with good clinical course and the patient was discharged to a long-term care facility within next 48 hours for further supportive care.
This case highlights the practicability and diagnostic utility of POCUS for the neurointensivist. Without POCUS, this patient’s cause of shock could not been narrowed down in a time efficient manner. Detection of the cause in this case preceded clinical signs of acute abdomen. Conventional diagnostic testing (echocardiography followed by computed tomography) would have not been able to narrow down the etiology in such a short time and could have been associated with high risk of circulatory collapse during transport. We encourage all providers in neurocritical care to learn basic critical care point of care ultrasound as a useful tool in improving patient care.
For further POCUS learning opportunities, please check out the 2018 Annual Meeting Workshops and sign up for the Critical Care Ultrasound workshop. If you are looking for volunteer opportunities at the workshop, please contact info@neurocriticalcare.org.
Figures
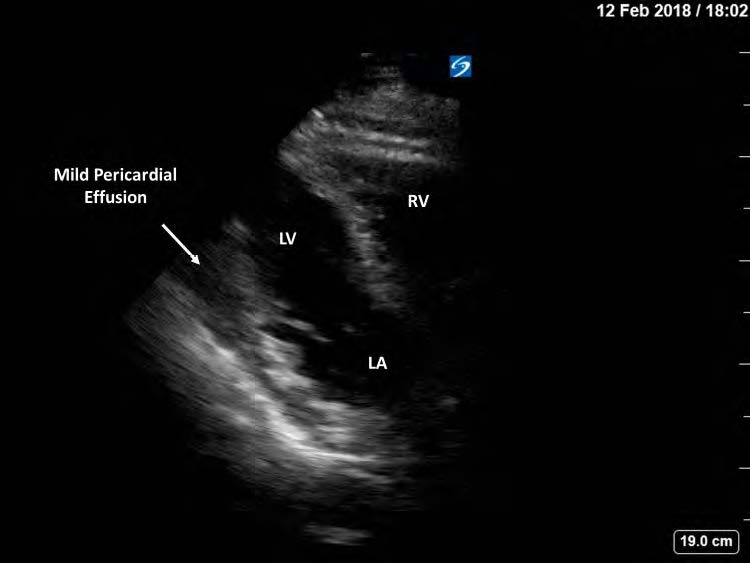
Figure 1. Limited transthoracic echocardiography, parasternal longaxis view, showing normal right and left ventricular morphology and function. LV stands for left ventricle; RV: right ventricle; LA: left atrium.
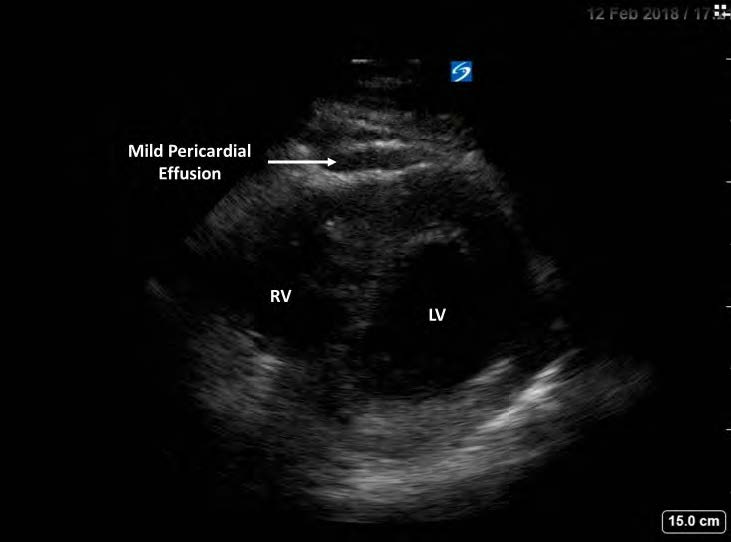
Figure 2. Limited transthoracic echocardiography, parasternal shortaxis view, showing mild pericardial effusion with normal right and left ventricular morphology and function. LV stands for left ventricle; RV: right ventricle
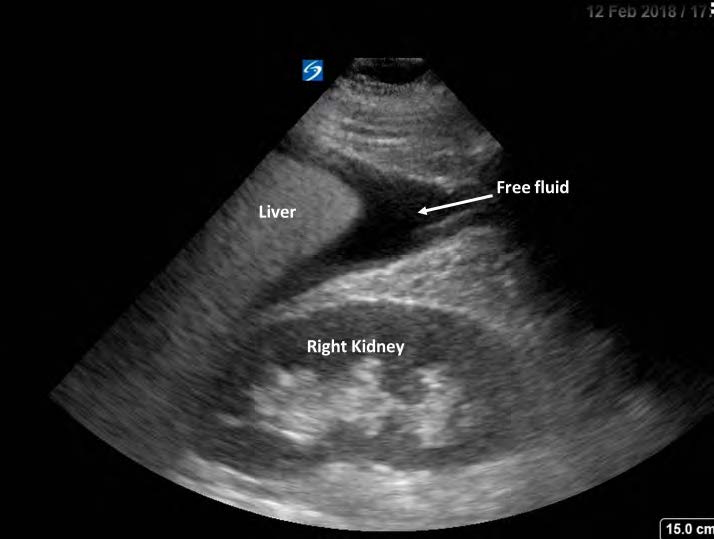
Figure 3. FAST exam, hepo-renal view, showing free fluid in Morison’s pouch.
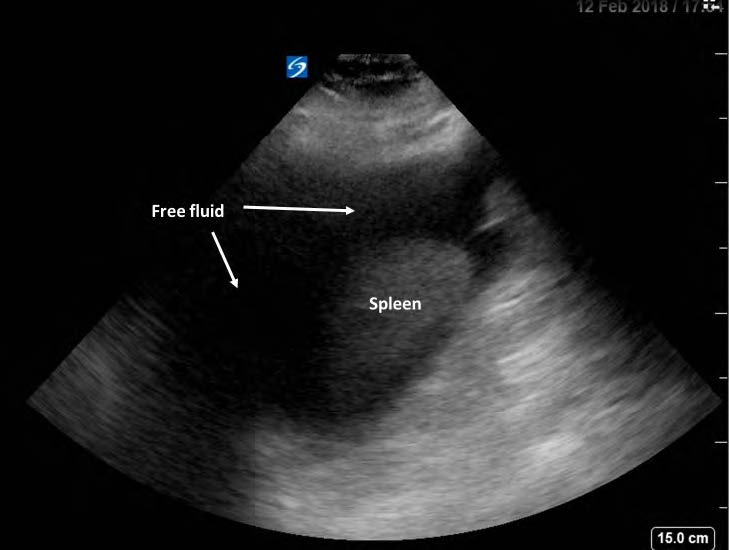
Figure 4. FAST exam, peri-splenic view, showing abundant free fluid around the spleen.
References
1. Zieleskiewicz L, Muller L, Lakhal K, et al. Point-of-care ultrasound in intensive care units: assessment of 1073 procedures in a multicentric, prospective, observational study. Intensive care medicine 2015;41:1638-47.
2. Royse CF, Canty DJ, Faris J, Haji DL, Veltman M, Royse A. Core review: physician-performed ultrasound: the time has come for routine use in acute care medicine. Anesthesia and analgesia 2012;115:1007-28.
3. Moore CL, Copel JA. Point-of-Care Ultrasonography. New England Journal of Medicine 2011;364:749-57.
4. AIUM practice guideline for the performance of the focused assessment with sonography for trauma (FAST) examination. Journal of ultrasound in medicine : official journal of the American Institute of Ultrasound in Medicine 2014;33:2047-56.
#LeadingInsights #POCUS