Incidental Finding of Hepatic Portal Venous Gas (HPVG) by Point of Care Ultrasonography
Published on: December 04, 2022
An 86-year-old male presented to our institution after a mechanical fall resulting in a large acute right-sided subdural hematoma with 1.5 cm midline shift. He was initially conversational but quickly deteriorated after CT scan, becoming obtunded with anisocoric pupils, L pupil 2mm reactive, R pupil 4mm non-reactive. He was intubated and underwent emergent craniotomy for evacuation of the hematoma. His medical history is extensive most notably for recurrent GI bleeds, also includes HFrEF (EF 35%), coronary artery disease, NSTEMI, paroxysmal atrial fibrillation not on anticoagulation, COPD, hypertension, abdominal aortic aneurysm, essential thrombocytosis (JAK2 positive, BCR-ABL negative) on hydroxyurea, and iron deficiency anemia requiring IV iron infusions.
The patient remained intubated post-operatively due to poor mental status, and had multiple episodes of dark brown emesis concerning for upper gastrointestinal (GI) bleed, for which the GI service was consulted. He was started on IV pantoprazole, although suspicion for active upper GI bleed was low due to a recent normal esophogastroduodenoscopy (EGD) and hemodynamic stability. His post-operative course was also complicated by acute kidney injury (AKI), for which the neuro ICU team applied point-of-care ultrasonography (POCUS) of the abdomen. There was no significant hydronephrosis noted and his foley was in place. However, an incidental finding of hepatic portal venous gas (HPVG) was found. Ultrasound revealed tiny echogenic spots or “bubbles” continuously floating through the hepatic veins into the inferior vena cava (IVC), see Figure 1. This was a concerning finding given that the most common etiology of HPVG is mesenteric ischemia1 and this patient was not receiving anticoagulation for atrial fibrillation. The patient had received a CT of the abdomen/pelvis as part of his trauma workup less than 24 hours prior to our POCUS which did not show any evidence of mesenteric ischemia or ileus. There was mild colonic wall thickening possibly reflecting colitis, as well as cholelithiasis with questionable mild mural thickening of the gallbladder. It is important to note that there was no evidence of bowel obstruction noted on the point-of-care ultrasound. A formal complete abdominal ultrasound was ordered the next day, which showed diffusely thick-walled gallbladder with stones and bile duct dilatation of 7-8 mm concerning for acute cholecystitis. There was no evidence of HPVG on this study. General surgery was consulted who recommended a hepatobiliary iminodiacetic acid (HIDA) scan, which did not show any cystic or common bile duct obstruction. No intervention was performed. The patient remained hemodynamically stable without any further episodes concerning for GI bleed. He was ultimately extubated and downgraded to the floor.
The radiologic finding of HPVG is rare, though historically a very ominous finding. In our case this was an incidental finding on POCUS. We chose to pursue further workup given the high association of HPVG with mesenteric ischemia, as this carries a mortality rate of 56-90%,2 is a surgical emergency, and for which the patient had multiple risk factors. In a study done by Liebman et al,1 after bowel necrosis (72%), the most common etiologies of HPVG are ulcerative colitis (8%), intra-abdominal abscess (6%), small bowel obstruction (3%), and gastric ulcer (3%). Gastric ulcer as the cause of this patient’s HPVG was a reasonable possibility given his history of GI bleeds and dark emesis during the admission. With the advancements in ultrasound technology and more widespread use of POCUS, HPVG is becoming more frequently reported. Often these cases do not have evidence of mesenteric ischemia nor do they require surgical intervention. McElvanna, et al. report three non-fatal cases of HPVG which were not due to mesenteric ischemia.3 One was due to acute pancreatitis which was managed conservatively, one due to post-operative intra-peritoneal hematoma following a Roux-en-Y hepaticojejunostomy for a benign biliary stricture, and one due to diverticulitis and septic thrombophlebitis. All three cases improved with conservative management (although there was surgical evacuation of the post-operative hematoma) and saw resolution of the HPVG.3
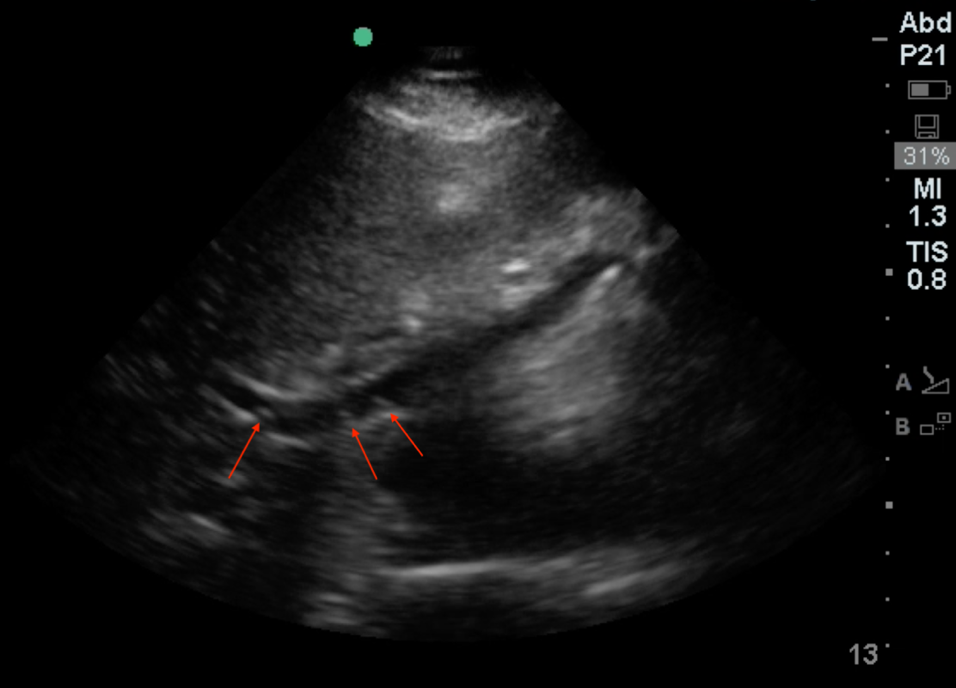
Figure 1. Echogenic "bubbles" of air floating through hepatic veins

Figure 2. Ultrasound clip of air bubbles floating through hepatic vein
The sensitivity and accuracy of sonography with doppler is comparable to CT scan,4 especially as an initial method for detection of HPVG, although in this case the finding on POCUS was not reproducible with formal ultrasound. Despite this, the neuro ICU team detected a rare, but perhaps increasingly more common, radiologic finding. Though HPVG is classically associated with mesenteric ischemia, a potentially devastating condition, it seems the differential has broadened to include more benign pathologies. This case shows that POCUS of the abdomen in the neuro ICU is a quick, easy, and inexpensive method of evaluating multiple organ systems to rule out acute pathologies. It serves as a useful starting point for pursuing more advanced imaging and surgical consultation. POCUS findings should be interpreted in the context of the patient’s clinical condition, hemodynamics, and other medical issues. Our review of the literature indicates that HPVG may not be as poor of a prognostic indicator as previously thought; however, it still warrants additional clinical consideration and workup.
References
- Liebman PR, Patten MT, Manny J, Benfield JR, Hechtman HB. Hepatic--portal venous gas in adults: etiology, pathophysiology and clinical significance. Ann Surg. 1978;187(3):281-287. doi:10.1097/00000658-197803000-00012
- Abboud B, El Hachem J, Yazbeck T, Doumit C. Hepatic portal venous gas: physiopathology, etiology, prognosis and treatment. World J Gastroenterol. 2009;15(29):3585-3590. doi:10.3748/wjg.15.3585
- McElvanna K, Campbell A, and Diamond T. Hepatic portal venous gas – three non-fatal cases and review of the literature. Ulster Med J. 2012;81(2):74-78. PMID: 2352685; PMCID: PMC3605538
- Nelson AL, Millington TM, Sahani D, et al. Hepatic portal venous gas: the ABCs of management. Arch Surg. 2009;144(6):575-581. doi:10.1001/archsurg.2009.88